Neural mechanisms and clinical distribution characteristics of herpes zoster
Herpes zoster occurs when the varicella-zoster virus reactivates and spreads along sensory nerves, resulting in localized skin lesions and neuropathic pain with a characteristic distribution. Recognition of the dermatomal pattern of involvement plays a crucial role in clinical diagnosis and in the prevention of postherpetic neuralgia.
Keywords: Herpes zoster; shingles; sensory nerves; neuropathic pain
Overview of herpes zoster (Shingles)
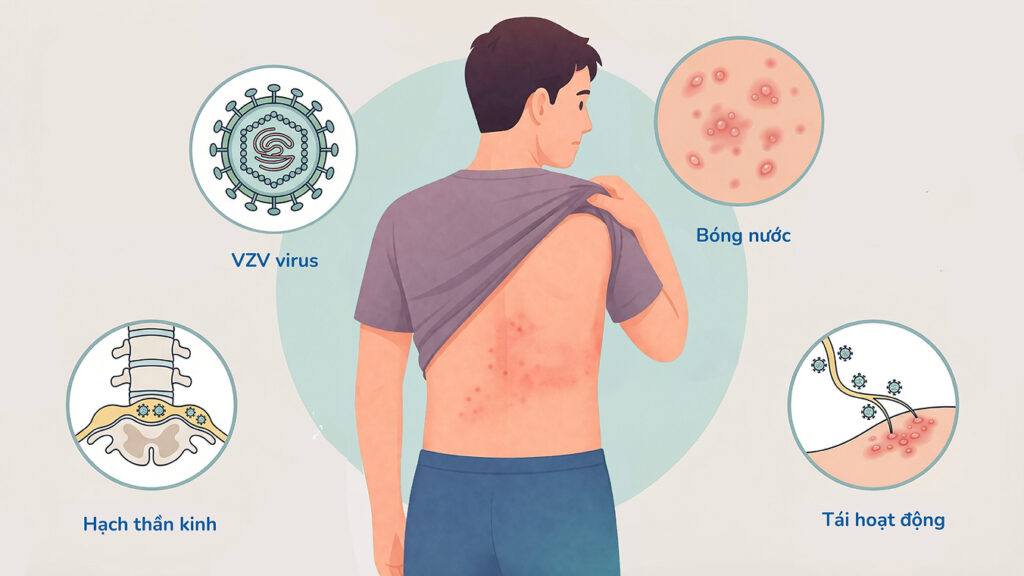
Herpes zoster, commonly known as shingles, is a viral infectious disease caused by the varicella-zoster virus (VZV), the same virus responsible for primary varicella (chickenpox). After recovery from chickenpox, VZV is not completely eliminated from the body but remains latent within sensory nerve ganglia, including the dorsal root ganglia of the spinal cord and the ganglia of cranial nerves. Under favorable conditions, the virus may reactivate and cause herpes zoster, which is characterized by neuropathic pain and localized skin lesions distributed along the territory of the affected nerve.
Overview of Herpes Zoster
Pathogenesis and neural spread of the virus
The pathogenesis of herpes zoster is closely associated with the reactivation of latent VZV within sensory nerve ganglia. When immune function is compromised or dysregulated, the virus begins to replicate within the ganglia and subsequently migrates centrifugally along sensory nerve fibers toward the skin. This process leads to inflammation of the affected nerves and corresponding damage to the overlying skin. Because each sensory nerve innervates a specific cutaneous region, herpes zoster lesions are typically confined to one or several adjacent dermatomes and characteristically appear on only one side of the body, without crossing the midline.
Dermatomal distribution and clinical significance
The dermatomes most frequently affected by herpes zoster are the thoracic regions, followed by the cervical, lumbar, and facial areas. When herpes zoster involves the face, it commonly affects cranial nerves, particularly the ophthalmic branch (V1) of the trigeminal nerve. This condition, known as herpes zoster ophthalmicus, carries a high risk of corneal damage, uveitis, and even permanent vision loss if not treated promptly. Therefore, dermatomal distribution is not only diagnostically valuable but also plays an important role in assessing disease severity and prognosis.
Clinical manifestations of herpes zoster
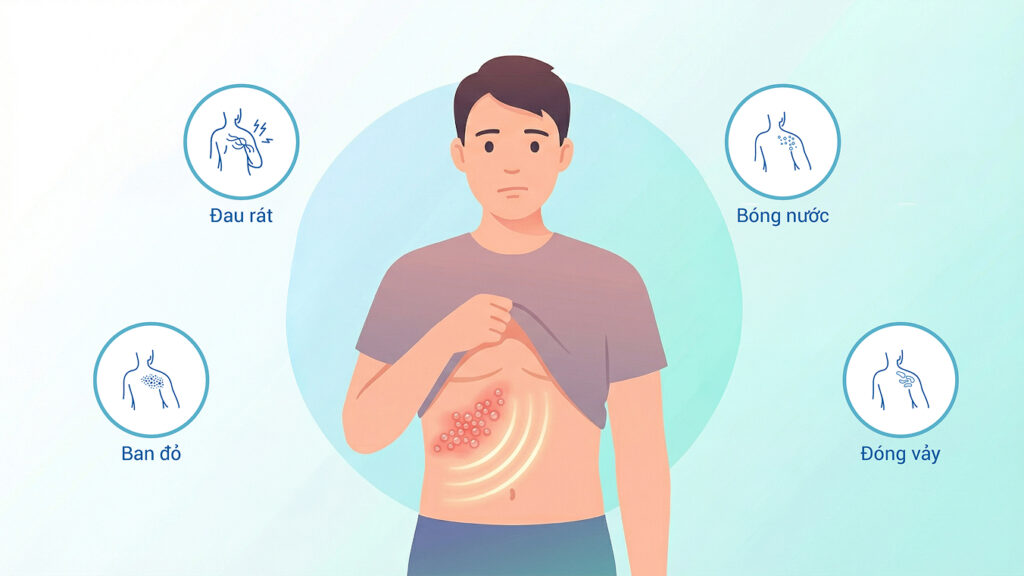
The clinical course of herpes zoster typically progresses through several stages. The prodromal phase is characterized by pain, burning, tingling, or dysesthesia in the affected skin area, often occurring several days before the appearance of the rash. The pain may range from mild to severe and is typically neuropathic in nature. This is followed by the development of localized erythema, which rapidly evolves into clusters of small, clear vesicles arranged along the affected dermatome. These vesicles may rupture, crust over, and heal within 2–4 weeks. In addition to cutaneous manifestations, patients may experience systemic symptoms such as low-grade fever, fatigue, and headache.
Clinical symptoms of shingles (Herpes Zoster)
Diagnosis of herpes zoster
The diagnosis of herpes zoster is primarily clinical, based on the characteristic combination of localized neuropathic pain and a vesicular rash distributed along a dermatome that does not cross the midline. In most cases, the typical clinical presentation is sufficient for diagnosis. However, in atypical cases such as those without vesicular lesions or in immunocompromised patients, laboratory testing, including polymerase chain reaction (PCR) analysis of vesicular fluid, may be performed to confirm the presence of VZV.
Treatment of herpes zoster
The goals of herpes zoster treatment are to reduce disease severity, shorten the duration of symptoms, and prevent complications. Antiviral therapy is the cornerstone of treatment, with commonly used agents including acyclovir, valacyclovir, and famciclovir. Treatment is most effective when initiated within the first 72 hours after rash onset. Supportive management includes analgesics, anti-inflammatory medications, and appropriate care of skin lesions. In severe cases, particularly those involving neurological complications or ocular involvement, corticosteroids may be considered under close medical supervision.
Complications of herpes zoster
The most common and concerning complication of herpes zoster is postherpetic neuralgia (PHN), characterized by persistent pain lasting months or even years after the skin lesions have resolved. PHN results from prolonged inflammation and damage to sensory nerve fibers. Other potential complications include localized muscle weakness, sensory disturbances, and rare syndromes such as Ramsay Hunt syndrome when the facial nerve is affected. Herpes zoster involving the ocular region may lead to serious ophthalmic complications if not managed promptly.
Prevention of herpes zoster
Prevention of herpes zoster primarily relies on vaccination, particularly with the recombinant herpes zoster vaccine Shingrix®, which has been shown to significantly reduce the risk of disease and related complications, especially in older adults and immunocompromised individuals. In addition, maintaining a healthy immune system and initiating early treatment upon symptom onset are important measures to limit disease severity.
References:
- Yetman, D. (2024, March 19). Nerve paths that shingles follows: What to know. Healthline. Medically reviewed by Shilpa Amin, M.D., CAQ, FAAFP, MSCP.
https://www.healthline.com/health/nerve-paths-that-shingles-follow - Cleveland Clinic. (2024, November 12). Shingles (herpes zoster): Causes, symptoms & treatment. MyClevelandClinic.org.
https://my.clevelandclinic.org/health/diseases/11036-shingles